
Technical Hospitality
Facing a post-antibiotic future, scientists and patients forge new alliances in pursuit of old therapies
How does one confront the creeping obsolescence of antibiotics? The answer might be at once future-facing and historical.
Antibiotics reveal surprising conjunctures. We live in a time where scientific techniques can reveal in increasingly fine-grained detail the properties of microbial species, some of which are pathogenic to human health. Yet, we are also increasingly incapable of remediating these pathogens with antibiotics due to their growing drug resistance.
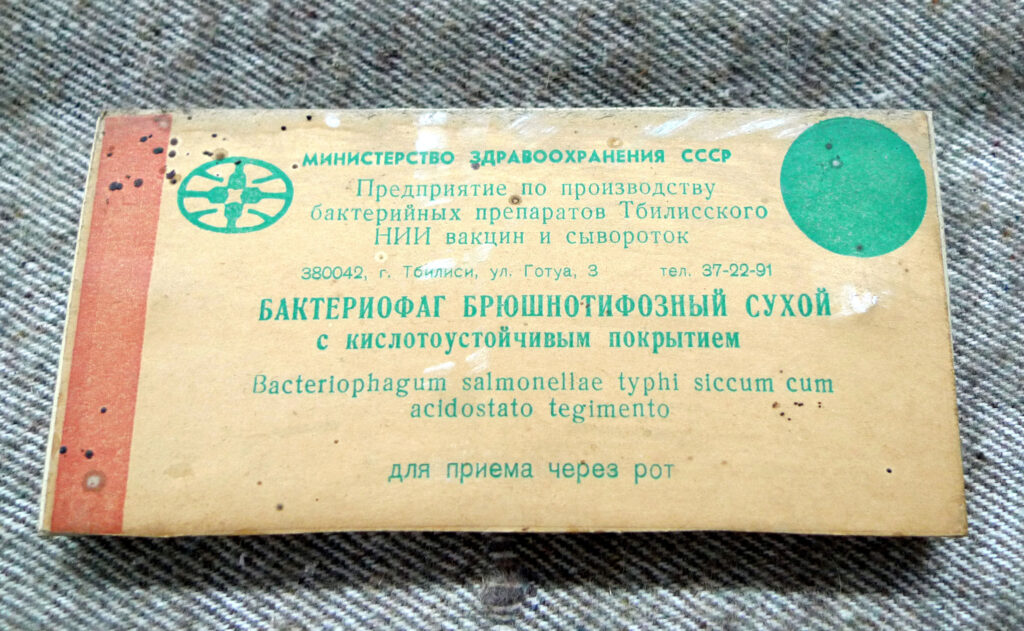
Antibiotics, long depended upon as an infrastructure of modern life, now confront obsolescence.1 Even as they have shown the way to health, they are becoming relegated to a crypt in which reside other moribund forms of therapeutic life. One such artifact is bacteriophage therapy, which deploys viruses that infect bacteria to achieve infection control. Traditionally associated with the Soviet imperium, phage therapy is now making a return in other parts of the world.
The idea of obsolescence permeates these conjunctures. It illuminates the limits of triumphalist knowledge and dominant techniques in the history of science and medicine. This pushes us to delve deeper into the lessons of time. Obsolescence harbors systems of thought that never rose to the level of established paradigms—but which, in time, might do so. Might one conceive of obsolescence also as a mode of revelation?
I

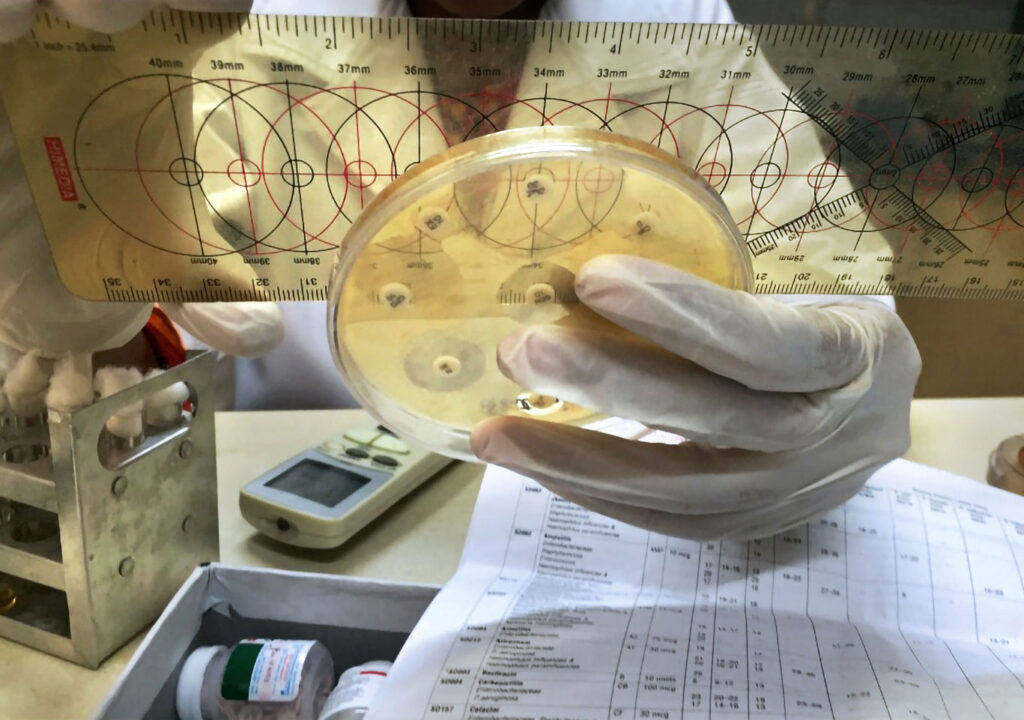
To find out, let’s journey to a laboratory in Delhi, where one can find clinical microbiologists on multiple quests to treat infections. Some grapple with manual, labor-intensive methods in which bacterial cultures are painstakingly grown on petri dishes, identified using microscopes and chemical reagents, and subsequently matched with appropriate antibiotics. Processes such as the disk diffusion method, considered gold standards in microbiology, require care and finesse on the part of lab technicians. Human judgment, here, remains key.
Other researchers here marvel at the affordances of tabletop devices such as GeneXpert and BioFire, often imported from the West and serviced locally. The technological prowess of such devices to rapidly know a pathogenic condition’s microbial etiology—that is, the source of what ails a patient—is belied by their ease of use. Increasingly pitched as “game-changers,” such devices—“locked and loaded,” as one operator put it to me—are giving stiff competition to older, slower methods.
This microbiology lab finds itself at a critical historical juncture. Today, its capacity to identify pathogens rapidly through automation confronts an increasing inability to address those pathogens with effective antibiotic treatments. On the one hand, the accelerating speed of understanding a microbe in the lab is celebrated. On the other hand, once-viable antibiotic drugs are facing failure at the hands of antibiotic-resistant superbugs. The arrival of advanced devices like GeneXpert and Biofire coincide with a rapidly diminishing medicine cabinet, one that is increasingly devoid of antibiotics that work.
What are the possibilities for medicine at a time when diagnostics struggle to translate into cures? For this microbiology lab in Delhi, a search for a more viable curative future manifests itself in journeys both epistemological and physical. This search demands humility and experimentation on the part of diagnosticians and patients alike—a willingness to recognize what is no longer working, to enlist the foreign and strange, to adopt into one’s future ideas that have long been discarded.
II
In response to growing disquiet in the realm of antibiotics, the Delhi lab is building new collaborative exchanges—of equipment, expertise, and experiences—with a unique Soviet-era facility, the Eliava Institute for Bacteriophages, Microbiology, and Virology in Tbilisi, Georgia. Here, the offerings are simultaneously historical and novel. They center on bacteria-devouring bacteriophage viruses, used extensively in the former Soviet Republic of Georgia but rendered moribund elsewhere due to a variety of technopolitical embargos during the Cold War.2
At their simplest, bacteriophages (known colloquially as phages) are viral predators of bacteria. Ecologically ubiquitous, these outlandish-looking objects accompanying bacterial hosts are the most widespread biological entities on the planet, and they are responsible for the culling of as much as forty percent of the planet’s bacteria daily. Invisible except under powerful electron microscopes, they typically measure one-millionth of an inch. Phage action takes place around and within us perpetually—even as you read these words.
If antibiotic resistance posits the end of a miracle that began with events in the early twentieth century—including the development of “magic bullet” drugs like salvarsan/prontosil and penicillin—the antibiotic era is increasingly revealed to be a blip in time: a medical exception.3 The relations between bacteria and bacteriophages, on the other hand, present a more eternal ecological dance. Staring into the creeping obsolescence of antibiotics thus reveals other national, ecological, and historical orders.
A microbiologist who hosted me in Delhi described her journey to the Eliava Institute as a return—as “bringing in the pre-antibiotic era in the post-antibiotic world.” We spoke often in the run-up to her 2019 trip to Georgia. We talked of travel logistics for Tbilisi and the difficulties that travelers, including medical migrants, faced at border control on the fringes of an increasingly xenophobic Europe. I shared places to stay and to eat, what to see while in the country, and where to get joyously lost once there. She reciprocated by offering a selection of scientific papers on contemporary phage therapy. These papers charted the emergence of new alliances in a post-antibiotic era. They also outlined potential perils in the mediation of phage-bacterial coevolution, and in the transference of novel resistance mechanisms between bacterial species. In one paper, my host had underlined the phrase: “Phage therapy is experiencing a well-deserved rebirth.”
For the lab in Delhi, forays into phage therapy represent an unfolding experiment. The hope, as my host put it, is that “traveling new paths will yield unusual miracles.” Bacteriophage diagnostics require testing a patient’s bacterial infection using the same culturing techniques that her lab in Delhi routinely conducts. Through these established diagnostic methods, the Delhi lab can forge fresh alliances—sensitivity patterns between a pathogen and its viral predator—to instantiate anew a cycle of human deliverance.
While my host was in Georgia, I received dispatches: images of her handling familiar equipment in novel ways, of electron microscopes, and of petri dishes demonstrating bacteriophage activity on lawns of antibiotic-resistant bacteria. There were images of the Eliava Institute’s old-timers as well as new recruits—managers and stewards of infection-control strategies after the Soviet era. There were pictures of my host bearing the weight of scientific heritage: there she was outside the institute’s columned archway, built in the tradition of Soviet high modernism that survived the collapse of the USSR; there she was next to Giorgi Eliava’s bust, built in memory of his scientific life and his death in the Stalinist purges. Accompanying these images was a letter confirming the institute’s invitation to this journey, physical, epistemological, and otherwise: ephemera of a nascent and potentially vital hospitality.
“The forging of this technical hospitality between ex-Soviet Tbilisi and contemporary Delhi tells a story of redressing past and future forms of obsolescence.”
Yet, what kind of hospitality is this? In his famous lectures delivered toward the end of his life, Jacques Derrida offered a typology of hospitality. On the one hand is the unconditional and unlimited reception of the stranger—radical and total openness. On the other is the “conditional law of hospitality,” where terms of conduct and conditions limit “radical heterogeneity.” Derrida’s point was that an ethic of responsibility demands continuous negotiations between the unconditional and the conditional, the open and the closed, heterogeneity and homogeneity; “One calls forth, involves, or prescribes the other.”4 The transgression of the conditional imperative of restriction and reciprocity determines the classification of the stranger no longer as a guest, but as an entity subject to removal. Yet, between the conditional and the unconditional there remains the negotiative realm: the realm of the necessary, that which must be done in order to live on.
III
Emergent forms of life, such as antibiotic-resistant superbugs, summon technical hospitality. This is the sphere of experimentation, and of reconsidering practices once cast aside. It is a reversal of old obsolescences, and a recognition of potential new ones. A future without viable antibiotics will bring many trials and tribulations, along with the usual challenges of scientific knowledge (and profit) production.
As they adopt the old-but-new paradigms of phage therapy, microbiologists, doctors, and patients will have to work through questions of legal ownership, scientific licensing, and biomedical regulatory approval. These hurdles may well strain the nascent hospitality emerging on this medical frontier. On the other hand, these pioneers all share in the pursuit of scientific knowledge for the sake of curiosity, bodily autonomy, and well-being.
My microbiologist host, bearing technical gifts, is a harbinger of a potential scientific return. Once characterized by diagnostic certitude and later by disquiet in the face of antibiotic failure, she and her colleagues have undertaken leaps of faith in pursuit of the bacteriophage. Working through this complex amalgam of obsolescences has required “a colossal working on oneself, with new experiences of the body, of movement, of being-together.”5
The forging of this technical hospitality between ex-Soviet Tbilisi and contemporary Delhi tells a story of redressing past and future forms of obsolescence. As the pendulum swings from the once-miraculous antibiotics back to the moribund phage, approaching one obsolescence means exiting another. Against fatalism and disquiet, technical hospitality demands journeys through peril—arduous inquiries into epistemology and embodiment that posit a space-time of a certain xenophilia: the love of the stranger, the guest, a virus that might just be a friend. ■

- Amid an array of news items in the popular press describing an incoming “antibiotic apocalypse,” see more process-oriented descriptions of the phenomenon in “Series on Antimicrobial Resistance: The Need for Sustainable Access to Effective Antibiotics,” Lancet, May 23, 2024, thelancet.com/series/antibiotic-resistance?; see also Kathryn M. Orzech and Mark Nichter, “From Resilience to Resistance: Political Ecological Lessons from Antibiotic and Pesticide Resistance,” Annual Review of Anthropology 37 (2008): 267–282. ↩︎
- Marc Landas, Cold War Resistance: The International Struggle over Antibiotics (University of Nebraska Press, 2020). ↩︎
- Søren Brøgger Christensen, “Drugs that Changed Society: History and Current Status of the Early Antibiotics: Salvarsan, Sulfonamides, and ß-Lactams,” Molecules 26, no. 19 (2021); Robert Bud, Penicillin: Triumph and Tragedy (Oxford University Press, 2007); Hannah Landecker, “Antimicrobials Before Antibiotics: War, Peace, and Disinfectants,” Palgrave Communications 5, no. 45 (2019). ↩︎
- Jacques Derrida, Of Hospitality (Stanford University Press, 2000), 147. ↩︎
- Achille Mbembe, Necropolitics (Duke University Press, 2019), 5. ↩︎